
Plugging a Leak
The Intricate Dance of the Coagulation Cascade.

**This article is not intended to diagnose or treat a disease. Consult your physician on questions related to your health.**
Intro
Hemostasis serves as the body's mechanism to prevent excessive bleeding. The process begins with primary hemostasis, resulting in platelet aggregation and the formation of a platelet plug. The final step, stabilizing the plug with fibrin, is achieved through the coagulation cascade. This article will review the entire process of hemostasis from injury to stabilized platelet plug for optimal healing. We will also spend a short time on different native and synthetic anticoagulants to finish this discussion.
Primary Hemostasis
When our bodies sustain an injury, the first set of actions encompassed in primary hemostasis results in a platelet plug. Primary hemostasis consists of four distinct actions: vasoconstriction, platelet adhesion, platelet activation, and platelet aggregation. Vasospasm and vasoconstriction are initiated when a blood vessel is damaged. The damaged endothelium exposes endothelin-1, collagen, von Willebrand factor (vWF), ATP, and inflammatory molecules. These various molecules, in turn, activate platelet adhesion. (1)
Platelets enter the injured area and adhere to exposed endothelium and vWF. Platelets bind to vWF with G protein receptors Ib-IX and become activated. Activated platelets undergo conformational change from smooth spheres to spiked with pseudopods. This activation also prompts platelets to release cytoplasmic granules. The cytoplasmic granules contain serotonin, platelet-activating factor, and adenosine diphosphate. Activated platelets begin synthesizing thromboxane A2, which promotes vasoconstriction and platelet recruitment. (1)
The cumulative effect of platelet activation is platelet aggregation. The GpIIb/IIIa receptors of activated platelets bind with fibrinogen and vWF. The fibrinogen begins forming cross-links, trapping platelets. This final step produces an unstable platelet plug and provides the environment to begin the coagulation cascade. (1)
Secondary Hemostasis
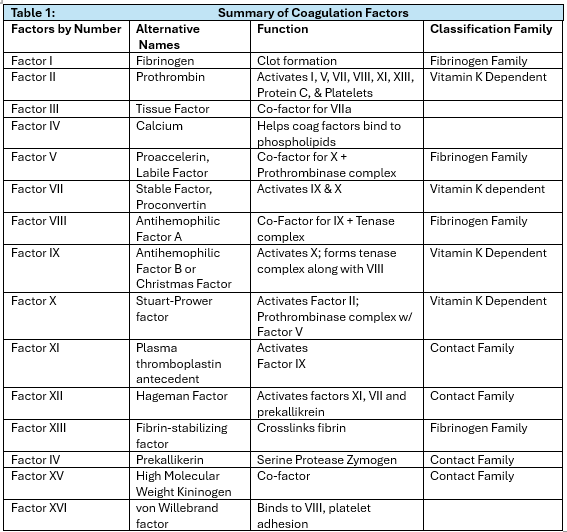
Secondary hemostasis aims to produce a stable platelet plug surrounded by a fibrin mesh. This process is accomplished through the intrinsic and extrinsic pathways, which converge to the common pathway. (2) Secondary hemostasis involves proteolytic enzyme factors (zymogens) and calcium ions. (3) The zymogens are designated as “factor” plus a Roman numeral but also have conventional names. Each activate factor (designated by “a” after the Roman numeral) becomes the enzyme that activates the next factor in the cascade. (3) See Table 1. The liver is responsible for producing most of the coagulation factors except III, IV, and VIII. (3) The coagulation factors can be classified by the pathway they participate in, which will be discussed later in this article. They can also be classified by unique characteristics such as the fibrinogen family, vitamin K dependent, and contact family. (3) See Table 1.
Intrinsic Pathway
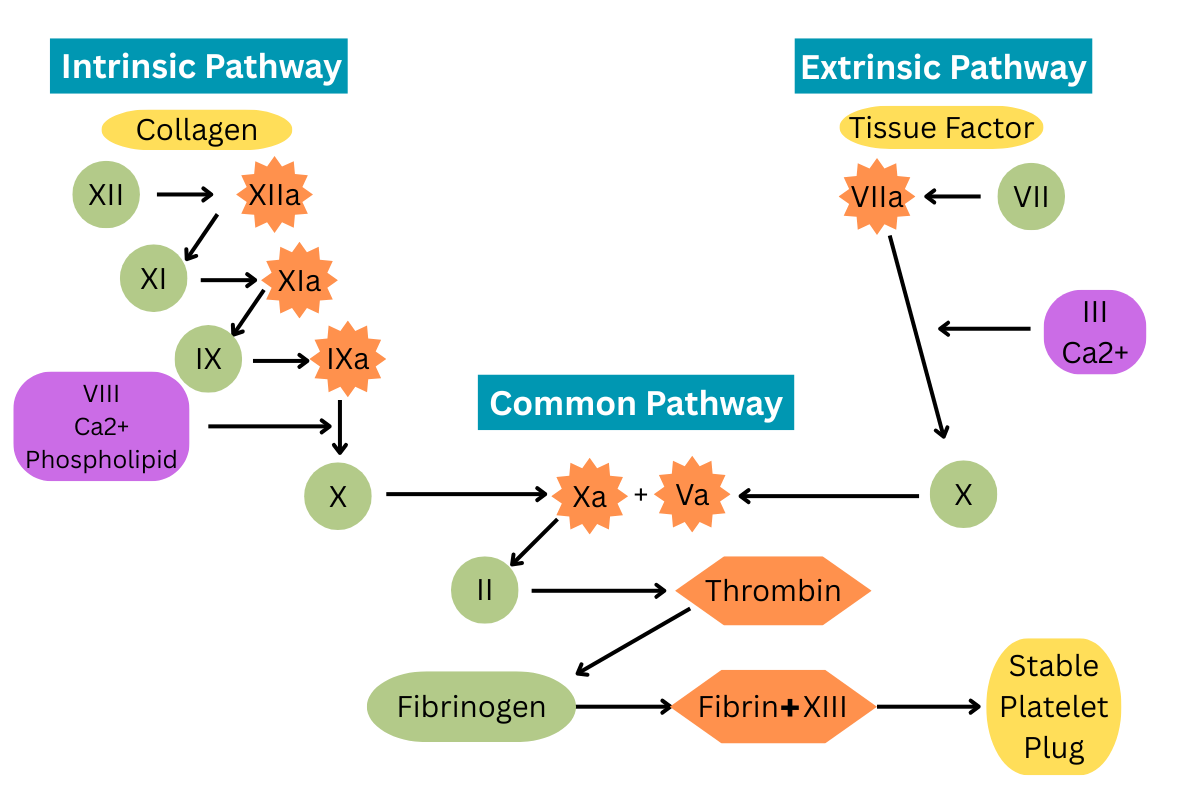
The intrinsic and extrinsic pathways are typically described as occurring independently. The reality is that they occur simultaneously and provide positive feedback for each other. To simplify, we’ll start with the intrinsic pathway. It begins with activating factor XII when it comes in contact with endothelial collagen. Factor XIIa catalyzes factor XI activation. Factor XIa activates factor IX. Factor IXa, along with factor VIII, calcium, and phospholipids, activate factor X. At this point, the intrinsic pathway is complete, and the common pathway begins. Let’s put a pause on the common pathway for a moment and explore the extrinsic pathway. (2)
Extrinsic Pathway
The extrinsic pathway is significantly shorter than the intrinsic pathway. After vascular injury, the vessel endothelium releases tissue factor. Tissue factor activates factor VII. Factor VIIa, factor III, and calcium activate factor X. This brings us to the convergence of the intrinsic and extrinsic pathways into the common pathway. (2)
Common Pathway
The common pathway takes us to the main objective of the coagulation cascade: converting the fibrinogen surrounding the platelet plug into stable fibrin mesh. Activated factor X and factor Va together activate factor II to thrombin. Factor IIa activates the conversion of fibrinogen to fibrin. Fibrin strands crosslink with factor XIII to form a strong, stable mesh around the platelet plug. (2)
Anticoagulation
Managing excessive coagulation is as crucial as hemostasis itself. This is achieved by several negative feedback loops that check the coagulation process at various stages. Thrombin encourages coagulation but also activates plasminogen to plasmin. Plasmin activates antithrombin, whose primary duty is fibrin degradation. Antithrombin also reduces the production of thrombin and the activation of factor X. Proteins C and S are also important internal anticoagulants. They are responsible for inactivating factors V and VIII.(2)
In some conditions, synthetic anticoagulants are essential to prevent excessive coagulation. These conditions include atrial fibrillation, deep vein thrombosis, major surgery, stroke, heart attack, pulmonary embolism, and unstable chest pain. There are four main classes of anticoagulants, each group acting on different parts of the coagulation cascade. Coumarins, commonly known as coumadin or warfarin, act by removing available vitamin K, thereby reducing the production of vitamin K-dependent coagulation factors. Factor Xa inhibitors, as the name indicates, bind with factor Xa and prevent its participation in the coagulation cascade. Heparins include unfractionated heparin, low molecular weight heparin, and heparinoids. Heparins bind with or inactivate factor Xa and thrombin. Finally, direct thrombin inhibitors bind to thrombin, rendering it ineffective. (4)
Final Thoughts
Hemostasis is an important process for preventing blood loss and healing. It is an intricate dance of enzymes, proteins, and calcium to form a stable platelet plug. Additionally, the body has innate mechanisms to prevent uncontrolled coagulation. When extra anticoagulant assistance is needed, synthetic anticoagulants can help.
Riddle Answer:
1. Vitamin K
References:
1. Garmo C, Bajwa T, Burns B. Physiology, Clotting Mechanism. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507795
2. Chaudhry R, Usama SM, Babiker HM. Physiology, Coagulation Pathways. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482253/
3. Palta S, Saroa R, Palta A. Overview of the coagulation system. Indian Journal of Anaesthesia. 2014;58(5):515. doi:10.4103/0019-5049.144643
4. Pope C BPharm, ed. Anticoagulants. https://www.drugs.com/drug-class/anticoagulants.html. Published November 22, 2024. Accessed February 27, 2025. https://www.drugs.com/drug-class/anticoagulants.html